
The Theory of Planned Behavior, originally proposed in 1967 by psychologists Izak Ajzen and Martin Fishbein as the Theory of Reasoned Action, remains one of the most widely-used psychological theories in the field of health behavior today. It's a classic for a reason -- its predictions have held up in hundreds of studies, it is intuitively appealing, and it is complex enough that much research can still be done around the edges. I have used the Theory of Planned Behavior in my own research, and I recently worked with two junior colleagues who are using it as the basis for their papers or grant applications. I truly do admire this model. The only problem, as I hope to demonstrate, is that it doesn't predict behavior.
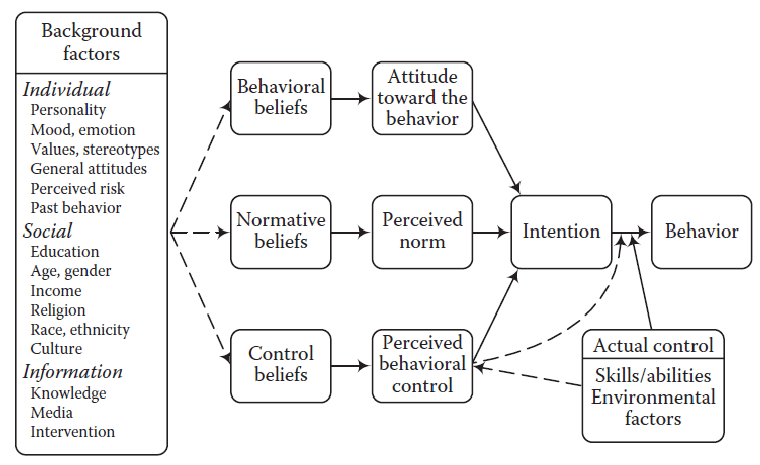
The basic theory, shown at the top of the page, proposes that people hold three different types of attitudes about a health behavior, and that each of these affects their level of intention to engage in the behavior. People's intentions are then expected to predict their actual behaviors. This is the classic version of the model, from around 1980. Although just one of the circles is labeled "Attitude," all three of the variables on the left-hand side of this diagram are actually attitudes or beliefs. They are mental representations about a behavior and its consequences. Further, they are
conscious attitudes or beliefs -- people can tell you what these attitudes are when you ask them. The same goes for intention to engage in a behavior, which people can report to you. Regular readers of my blog will see where this is going: Attitudes and beliefs that can be expressed in language are generally
products of the Narrative Mind.
What are the three kinds of attitudes? The person's
attitude toward the behavior is sometimes described as an
efficacy belief or
outcome expectancy. In other words, if you engage in the behavior, what results will that produce? It can include both the desirable and undesirable outcomes of a behavior -- i.e., therapeutic effects and side effects. I might believe, for instance, that exercise will reduce my long-term risk for heart disease (which I like), and also that it will make me sore and sweaty (which I don't like). Together, that mix of beneficial and adverse effects makes up my attitude toward the behavior itself, which on balance can be positive or negative. An attitude is a narrative: It is my conscious evaluation of the properties of the behavior, whether or not I like it, and why.
The second component of the Theory of Planned Behavior,
subjective norm, reflects my belief about how
other people see the behavior. A widely cited example is that college students who drink heavily also say that 90% of their peers drink heavily, even though the objectively measured rate is closer to 10%. For purposes of the model, it doesn't matter what the true state of affairs is, only the person's perception about it. The subjective norm component includes the emotional evaluation that is called
valence in the older
Health Belief Model -- whether a behavior is good, bad, or indifferent. In the Theory of Planned Behavior, your personal, internal evaluation of a behavior is seen to be tied to your mental model of how other people see that behavior. That's why the "norm" label is used here. Again, regular blog readers will recognize
social perception as a key function of the Narrative mind: In
Jonathan Haidt's useful metaphor, the Narrative mind is the "rider" on top of the "elephant" of the Intuitive mind, shouting out explanations and apologies as the elephant lumbers around, managing social interactions so that the other riders and elephants won't get mad at us.
Finally, the
perceived behavioral control component is very similar to the idea of
self-efficacy in
Bandura's Social Cognitive Model of behavior. It represents the extent to which people believe they can change their behavior, what the external barriers are, and their evaluation of their own capability to make changes. Behaviors that are seen as beyond our control or at the mercy of circumstances are less likely to be tried. People differ in their beliefs about whether they can influence an outcome; as with the concept of subjective norm, the person's belief matters more than their actual ability. As in the saying attributed to Henry Ford, "whether you think you can, or you think you can't, you're right."
The Theory of Planned Behavior shown above was already an evolution from an earlier theory. The original Theory of Reasoned Action was slightly simpler, without perceived behavioral control. It also had some "precursor" concepts, that were related beliefs (ideas, postulates, factual statements) that led to the more emotion-laden attitudes as a second step. This was in the time of the cognitive revolution in psychology, when psychologists were focused on changing people's beliefs as a way of affecting their behavior, so the initial emphasis on factual beliefs makes sense. As time went on, emotion-laden attitudes took on more importance, and these were empirically proven to have a closer relationship to the ultimate outcomes of intentions and behaviors. Therefore, the precursor beliefs don't appear in the later model shown at the top of the page. (As we will see below, though, the authors never gave up on this idea).

Something that I always appreciate about the Theory of Planned Behavior is its creators' humility in modifying their work as new evidence became available. It was just around the same time as the Theory of Reasoned Action that Albert Bandura's self-efficacy concept began to generate great excitement in the literature. Ajzen and Fishbein tried adding Bandura's measure to their own studies and discovered that it added explanatory power, so they revised and renamed their model to include the third attitude construct. A second modification came later, in the form of a dotted line between perceived behavioral control and behavior: Ajzen and Fishbein found that self-efficacy not only predicted intention, it also directly predicted behavior to some extent -- the only one of the model's constructs that does so. This can be explained based on a certain level of agreement between people's perceived control over their behavior and their actual level of control. To the extent that perceptions of control are accurate beliefs, they are simply predictions about whether an attempt to change behavior will succeed or fail. And indeed, the original concept of self-efficacy has been found to consist of both a reality-based predictive element and a perception-based subjective component. Here's a different version of the Theory of Planned Behavior that includes actual behavioral control as an external factor that can either augment or enervate the effects of perception. Perceived difficulty is another way of describing the idea of a person's actual control over a behavior. Sometimes this concept is included in modern iterations of the Theory of Planned Behavior and other times not, but the dotted line between perceived control and behavior is usually there.

In a third iteration of the model around 2001, Fishbein brought back some of the precursor constructs, this time applying them to all three of the attitude types. There are conveniently two precursors for each attitude -- symmetry and elegance being other appealing aspects of this theory!
This version tells us something about where a person's attitudes might come from. Besides outcome expectancy (behavioral beliefs), a person's attitude toward a behavior also depends on their thoughts about what other options might be available. In other words, what is the best alternative? The precursors for subjective norm involve both normative beliefs (what will other people say?) and the person's level of motivation to comply (what will other people actually do, if I engage in the behavior or not?). I like the motivation aspect, again because I think it fits well with
Haidt's work on motivated reasoning, and also because I generally see an important
role for motivation in predicting behavior. Finally, perceived behavioral control arises from beliefs about one's power to engage in the behavior (i.e., control beliefs or self-efficacy) and their perceived power (i.e., even if it's under their control, do they have the "oomph" to actually get it done?). Again, these seem like logical extensions of the model, and they give health psychologists more potential points at which to intervene by convincing someone to change their beliefs.
What about individual differences between people? Here's a fourth version of the model -- perhaps the most current? -- that acknowledges the effects of demographics, personal history, health literacy, and social determinants of health on someone's initial beliefs. Those beliefs in turn inform their attitudes, their attitudes inform their intentions, and their intentions (together with their actual level of control over the situation) predict their behavior. In this version the precursor beliefs are back to being one box each, although one could argue that the subsets of beliefs behind each type of attitude are still implied. The box on the left is an "... and the kitchen sink" type of list, which basically says that a lot of things about a person's biology, social determinants of health, past experiences, and knowledge base can all play into their attitudes. It's more of an acknowledgement that the model doesn't predict everything than a strongly useful set of predictors. But somewhere in that list might be an additional factor that the next up and coming scholar could use to further develop and refine this highly popular model.

What, then, should we make of this model? It's quite a bit more complicated than it was back in the Theory of Reasoned Action days, but the basic relationships between variables have remained essentially the same (the exception being that direct link between perceived control and behavior). In fact, once
actual control is included, the relationship between perceived control and behavior
isn't very strong -- the degree to which perceived control affects behavior is the degree to which one's perception is true. Adding more or different variables on the left side of the model just takes us further upstream; the only way to get from those variables to actual behavior is by way of intention. We are left with a wide range of beliefs or attitudes that we might want to help people to change, but unless making those changes affects their ultimate intention to engage in a behavior, those changes don't really get us anywhere. It's still quite possible to have a patient who knows what they ought to do, but doesn't do it.
The last arrow in all of these diagrams is the
weak link in the model, as noted in 2003 by Dr. Jane Ogden. Oh, don't get me wrong: There is indeed a statistical relationship between intentions and behaviors, which has been borne out in numerous meta-analytic reviews. Here's how that significant relationship is achieved. Imagine 100 people, half of whom intend to exercise and half of whom do not. We then follow those people for a month, and find out how many of them actually achieved their exercise goals:
Actually Exercise
Intend to Exercise NO YES Total
NO 45 5 50
YES 25 25 50
Total 70 30 100
This table shows a highly statistically significant relationship between intention and behavior (chi-square = 17.2, p < .0001), a fact that Ajzen and Fishbein rely on in their
response to Odgen's critique. The odds that a person will exercise are indeed five times greater if they say that they will exercise than if they say that they will not. But consider the bottom row, the case in which someone says they will exercise. In that case, the prediction of whether they will actually exercise is
no better than chance. The conclusion, then, is that someone who says they do not intend to exercise is usually accurate. But someone who says that they
do intend to exercise is as likely as not to be wrong.
Are we surprised by this result? If we are honest about the relationship between our own intentions and our own behaviors, probably not. (What's more surprising, truly, is the small number of people who
didn't intend to exercise and yet end up doing so). If we are trying to use intention as a predictor of behavior, what we most want to know is whether someone who says they
will exercise is going to carry through on their intentions. And the answer, in numerous Theory of Planned Behavior studies, is that we simply don't know. In fact, people
themselves probably don't know -- they genuinely intend to, but neither they nor we have any way of knowing what will really happen. The reason for this is that every element of the Theory of Planned Behavior is
commonly measured at the level of the Narrative Mind. And the
most important statement in Two Minds Theory is that the Narrative Mind does not control behavior.
I do love the Theory of Planned Behavior. It is an excellent model if your goal is to predict intentions. But if your goal is to predict actual behavior, it comes up short. Like many health behavior theories, it falls straight into the "intention-behavior gap," and its problems can't be fixed with any solution that studies behavior at the level of the Narrative Mind.




Comments
Post a Comment